Countless studies have shown that games are a preferred and effective tool for training1, but can video games impact doctors’ decisions in actual clinical scenarios? What about for busy physicians with 14 years of experience under their belts?
The answer is a resounding “Yes,” to both questions, according to a groundbreaking study of practicing doctors. The analysis found that medical video games increase the clinical competence of busy, experienced physicians and enhance their decisions in relevant medical scenarios.
The first-of-its-kind, third-party study assessed doctors who played Level Ex’s Top Derm, a video game developed for dermatologists that includes focused challenges across a range of dermatologic images and case scenarios. For the study, physicians played five Top Derm game modules that address common and rare skin disorders.
Players’ knowledge attainment was studied during the games and their knowledge retention and transfer were analyzed weeks later, when doctors were presented with new patient case scenarios that assessed the same knowledge in a completely different format than what they had experienced in the game.
Across all modules, all players of all experience levels and ages showed a statistically significant score improvement in the post-knowledge assessment. Among three modules—Zebra Cases (referring to skin disorders out of the ordinary), Visual Skinsations (addressing hair and scalp disorders), and Pesky Pimples (pertaining to acne conditions)—40% of physicians demonstrated improved knowledge in the post-assessment.
When presented with the patient clinical scenarios, 88% of players either retained or improved their score across the three clinical modules.
Novel Findings
The findings are especially novel because of the hard-to-reach and rarely-measured demographic.
Doctors in the study ranged in age from 32 to 57, with an average of 14 years of practice experience. Past studies on medical video games have primarily centered on students and residents. These studies analyzed outcomes such as preference over traditional CME and players’ knowledge improvement compared with control groups.
Clinical competency increased among older and young doctors alike, and neither age nor experience showed a relationship with score improvement.
How did doctors’ thinking change?
In one patient scenario, for instance, 10% of physicians changed their management of acne during pregnancy after playing Top Derm. In another scenario, more doctors correctly changed topical acne treatments to improve efficacy and decrease resistance based on their game experience.
As reflected in prior studies, a large majority of doctors found medical video games more enjoyable than traditional continuing medical education (CME). Nearly 75% of the physician players said they preferred learning through play over CME. This affinity was consistent among all ages and experience levels.
Comments from doctors included that the format was “easy to use,” included many “great teaching exercises” and fueled “stimulation of thought.” The game was also described as, “fun, clinically relevant, and easy to do in spurts.”
Doctors chose to spend more time in the modules where they had the least prior knowledge, according to the study. Overall, players improved their in-game scores by up to 24%, depending on the pack’s dermatology topic.
This landmark study proves that medical video games can improve the applied clinical reasoning of busy, practicing doctors and that those improvements are measurable weeks later, in distinct clinical scenarios far removed from a video game context. These milestone findings suggest sharper diagnoses in the exam room and better care for patients.
The Top Derm study was developed and conducted by CE Outcomes LLC, an independent, educational research firm that specializes in continuing education and medical information resources for clinicians and patients.
My ongoing exploration into the inner workings of ChatGPT has brought me to a crucial understanding that many don’t realize:
ChatGPT’s implementation is shockingly…mind-blowingly… simple.
It joins other such mysterious phenomena of “unimaginable complexity emergent from incredible simplicity” that the human mind struggles to comprehend… like how a short DNA sequence that could fit on a CD encodes a complete human.
When folks hear stats like “terabytes of training data” and “175 billion parameters” they think “wow – this thing is super complicated!”. That impression is completely wrong. The “engine” that is ChatGPT is so incredibly simple, even I struggle to believe that it produces the output that it does.
Seeing ChatGPT in-action helps us overcome our innate biases that limit our understanding of how memory works (and how the human brain works in general.)
I’ll explain.
Understanding ChatGPT’s Inner Layout
ChatGPT is surprisingly willing to share the details of her architecture. In my prior “interviews” with her, I’ve collected all the data necessary to calculate her layout and complexity below. Another interview (here) verified a few assumptions that I had made.
To understand ChatGPT’s inner workings follow these 3 steps:
1. Imagine 2 million dots.
Actually, you don’t have to imagine them. It’s the number of pixels in a 2 megapixel photo (your iPhone defaults to 12 megapixels.)
They fit onto a small image. Here are 1 million dots, so imagine two of these images:
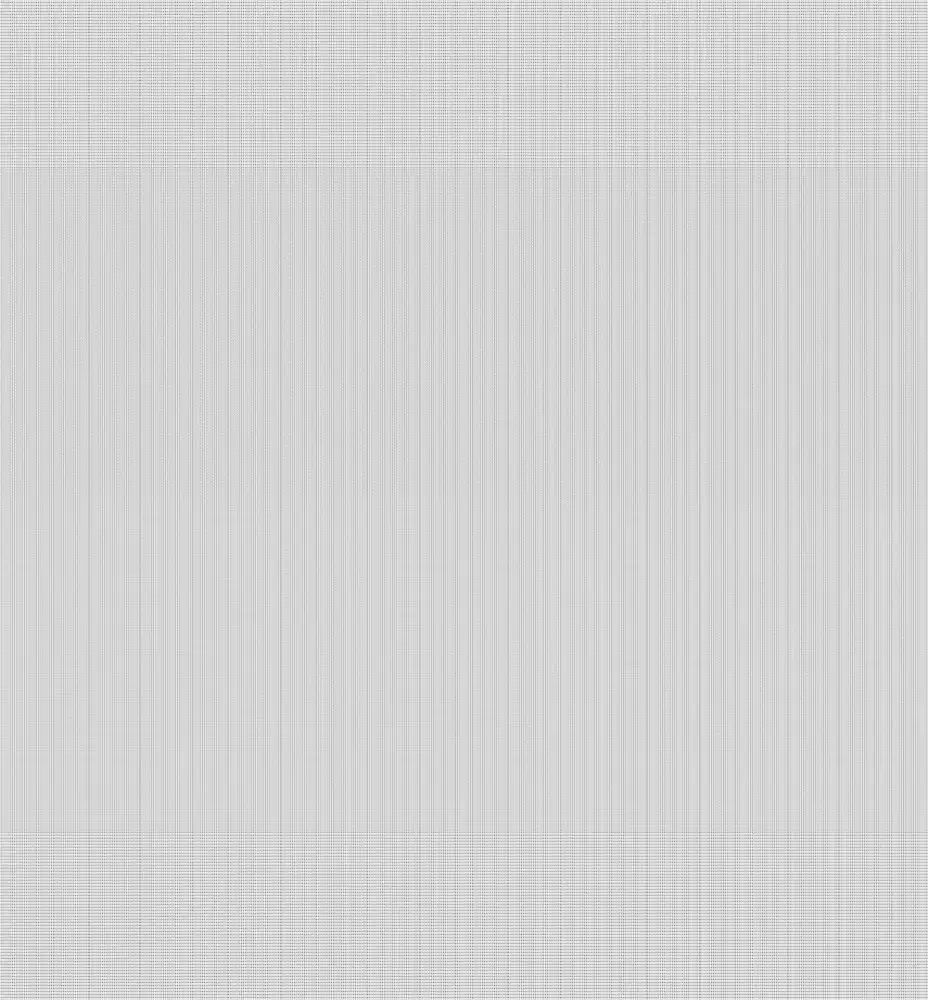
2. Rearrange those dots so they’re in 24 long rows, about 85,000 dots wide
3. Now for each dot, connect it with every dot in the next row by virtual wires of varying thickness, like this:
You will have ~175 billion wires. The thickness of those wires represents 175 billion numbers. Those are the “175 billion parameters”.
Those dots are all exactly the same – they “perform” incredibly simple math in an artificial neural network, taking the input from the previous layer and multiplying it by the parameters (wire thickness). The idea is to sort of approximate the way a simple biological neuron works: the wires represent the neural connections.
THAT’S IT.
I’m not kidding. That’s it.
There is no database. Not a single text file. No documents. No backup copy of Wikipedia. No internet connection. No folder full of manuals. Just 175 billion numbers, laid out like a weaved scarf. Just those numbers. It would fit on a 256GB USB stick with room to spare. That’s it.
All of the logic, the “intelligence”, the quotes, the humor, the names – all of the product manuals, the bible, the shakespeare… everything that informs ChatGPT’s output is encoded and added (by its learning process) into the layout above. That’s it.
“But Sam, doesn’t it also have a…?”
No. No it doesn’t. That’s it.
What about all of the things that I tell ChatGPT in the chat?
If you aren’t blown away yet that all of ChatGPT is just 175 billion numbers, wait until you hear this: your entire conversation with ChatGPT, no matter what, is represented by 2,048 numbers. No more.
When you “talk” to ChatGPT, it takes the letters you give it and encodes them into up to 2,048 values, and it puts those values into the front end of the network above. The output of the network is its response. If you enter more than 2,048 letters (like when you paste in a long article or a manual), it grabs the first 2,048 letters, runs it through the network to generate a ‘hidden state vector’ that is 2,048 numbers long, and combines it with the next 2,048 letters and runs it again (this is a slightly simplified explanation of the algorithm but not much).
That’s why ChatGPT doesn’t learn from your conversation. Every conversation is from scratch. Those 2,048 numbers change during a conversation. The 175 billion numbers don’t change no matter how much you talk to her. Those numbers only change during a ChatGPT upgrade.
What this means
This ranks ChatGPT among a category of “unimaginable complexity emergent from incredible simplicity” that we see in certain natural phenomena, and once in a while in computer science. Here are some other examples:
DNA – 4 billion DNA nucleotides is 691 megabytes of data. That fits on a CD. It represents a human. Change enough numbers, you get a tyrannosaurus instead. Or a jellyfish. Or a rutabaga.
Fractals – Fractals in math and in nature take a simple mathematical equation and repeat it at progressively smaller scales, creating self-similar shapes that are infinitely complex. The simplicity of the equation belies the complexity of the shapes it generates.
Cellular automata – Cellular automata (examples here) illustrate how a simple set of rules can create a wide range of complex patterns and behaviors. By updating the state of each cell in a grid based on the states of its neighbors, cellular automata can produce intricate and dynamic patterns that can appear to be alive and seemingly intelligent.
Demoscene – An emergent subculture in computer graphics – demoscene is a category of tiny programs written by skilled experts. A program made up of 4 kilobytes (or smaller) generates gorgeous, complex, animated worlds.
The human brain – and beyond
For years, many of us struggled to believe that human memory could be encoded in neurons and neural connections (“there has to be something more!”)
In my view, seeing the emergent behavior from ChatGPT puts those objections to rest. Seeing ChatGPT in-action helps us overcome this and other innate biases and preconceptions that limit our understanding of how memory works (and how the human brain works in general.)
We’ll explore implications for brain research in future articles.
This article was written by Level Ex CEO Sam Glassenberg and originally featured on LinkedIn
You can’t wait to build this game. After meeting with Level Ex, you’ve decided on a concept that’s going to extend HCP engagement and highlight your brand’s differentiation to drive adoption. It’s going to light up all the right parts of the brain—rewarding and memorable. You’re eager to get this game in front of your HCPs, but a lingering concern gives you pause: the MLR review process. If you’re wondering how a video game makes it successfully through the rigor of MLR approval, this post is for you. Below, Senior MLR Product Manager Rachel Mansfield shares her strategies for a seamless review process, ensuring approval.
Rachel leads with 23 years of combined experience in agency marketing compliance management, content and design marketing, and project operations. Her role is unique in the life sciences industry–as she leads the only dedicated MLR team embedded in a video game studio. With an unmatched track record of successful MLR approvals, Rachel understands the many unique considerations involved in bringing interactive game content through medical, legal, and regulatory review.
Q: What kind of medical games do healthcare companies create with Level Ex?
We make games that improve the way medical professionals identify, diagnose, and treat patients. We do this across a dozen different therapeutic areas, such as dermatology, gastroenterology, oncology, and cardiology. This includes everything from diagnosing rare diseases on skin of color to performing virtual surgeries collaboratively. Healthcare companies come to us to help doctors understand the benefits of their products and how to use them properly.
Q: How many MLR assets are you bringing through approvals every year?
I’ve guided successful MLR processes with more than 30 different pharmaceutical and med device companies, receiving MLR approval from over 90 different brands, and more than 500 assets annually. Level Ex has launched a plethora of customized branded and unbranded professional gaming experiences for our clients. At any given time, we have around 20 projects in the MLR review/approval process.
Figure 2: Our MOA solution was designed for MLR compliance. Want to play? Click here to play and interact with our MOA solution!
Q: At what point do you and your team get involved in the MLR process?
At kickoff, I familiarize myself with the specifics of the brand or medical device and all things MLR-related. Once we have developed the content with the brand team, and a storyboard, my team reviews, substantiates, and contextualizes the content before submission. From there, we handle the submission and implement any changes, ensuring that our product is properly prepared for review by our client’s MLR team. If possible, we even like to attend all live review meetings to provide necessary context and answer questions as they emerge. By doing so and asking the right questions on the front end for preparation, we set our clients up for smooth, successful approvals.
Q: What are the different submission systems you work with?
Most agencies do not have an MLR team, which generally designates the submission responsibility to their marketing team. Level Ex has dual capabilities: direct management and submission or stewarding the submission with our clients. We are the only video game studio trained and certified to submit materials directly to an extensive list of pharmaceutical companies through their review platforms such as Veeva Vault PromoMats and FUSE.
Q: Let’s talk about timing. What happens if an MLR approval takes too long? Or if another MLR review is required?
In a perfect world, approval never takes too long and additional reviews aren’t needed, but we know that’s often not the reality. We understand the complexity of preparing assets for approval, and we’re more than prepared to smooth out any wrinkles and maintain momentum. Our development team follows an agile methodology, so if an asset is held up by review, the team knows how to identify and eliminate the stopping blocks to keep a project moving forward. This is one of many areas where being all-digital is a major advantage—we can make updates to elements like ISI with ease. We design our game mechanics and tools to accommodate a wide range of typical MLR requests such as adjusting scale, ISI positioning, sequencing, branding, and more.
Q: What are some of the obvious considerations that you plan for?
Our MLR team reviews, substantiates, and contextualizes all promotional assets prior to submission. We’re proactive throughout every aspect of the planning, development, and MLR submission to ensure a seamless review and approval process. For example, for any first-time clients or new products we develop, our team proactively adds a concept review with the regulatory team to the timeline. Doing this ensures that we address any concerns or red flags early, which drastically reduces any content, design, or development rework at a later stage. We also repurpose pre-approved content when possible and collaborate closely with the brand team to ensure a successful MLR approval.
Q: How does Level Ex balance the structure of MLR with the fun of playing a game?
It may sound strange, but as a team of game creators, we love rules. Rules are what define a game and set the balance between fun and challenge. Can you imagine checkers or chess without the rules that determine how each piece moves? So we actually embrace the rules that come from medical, legal, and regulatory confines. Some of our best—and most effective—designs come from constraints.
Want to see more? Have additional MLR-related questions for Rachel and our team? Contact us.
I had a fascinating “interview” with ChatGPT last night, exploring her overall architecture and computational complexity. I don’t have a background in machine learning, so my questions clearly come from the background of somebody with a background in general CS, computer graphics and GPU architecture.
We explored things like algorithmic complexity, data representation, and comparison to Midjourney and other systems. I learned a great deal about how this all works.
In one or two cases, she gave a response that sounded like it might be incorrect. When I called her on it, I think she actually acknowledged the error and updated her response.
A few things I learned (full explanation in the interview):
GPT3 has 175 billion parameters (ANN connections). 12 neural layers in the encoder, 12 in the decoder. Each layer is made up of two sub-layers: a multi-head self-attention mechanism and a position-wise fully connected feed-forward network. Input vector size is 1024.
Trained on terrabytes of text data
It is a fully connected neural network, also known as a dense network, each node in a layer is connected to every node in the previous and next layers
It’s based on Transformer Networks – a type of neural network architecture that was introduced in a 2017 paper by Google researchers called “Attention Is All You Need”. Training is done via TensorFlow and is GPU accelerated via CUDA and OpenCL.
Computing model parameters involves a sparse matrix solver implemented using Gradient Descent. Sparse matrices are represented in CSR format in memory.
Specific techniques/approaches discussed: Masking, Transformer Networks, Transfer Learning, TensorFlow, Floating Point to Integer Quantization, Loss Functions, Attention, Self-attention, Multi-head attention, backpropagation, word embeddings
ChatGPT’s word embeddings are a black box, represented as dense, high dimensional vectors. They don’t use word2vec. There are millions of embeddings.
There are no adversarial neural nets involved – that’s specific to DALL-E and Midjourney
By very rough calculations, ChatGPT performs 10^9 or 10^10 neural calculations per second. The human brain is estimated around 10^16. It’s obviously not an ‘even’ comparison, however.
Here are some example questions from my ‘interview’:
Are you based on adversarial neural networks?
Can you give me an example of how this would work using a specific sentence (or set of sentences) as a training example?
Does your neural network change at all during usage? Or is it static?
Do you use transfer learning? How?
How large is your dataset ?
How large is your neural network ?
Walk me through how your training works at the GPU level?
Are the GPU computations done in integer or floating point?
What does the loss function look like?
What does the loss function look like for language translation? Give me an example?
What neural network features do you use ? Backpropagation, for example.
What do you mean by “attention” in this context ?
How many nodes are in these neural networks ? How many layers?
What do you mean by fully connected?
How are these sparse matrices represented in memory?
What does a word embedding look like? How is it represented? Can you give me an example?
How would you compare the number of neural calculations per second to that of the human brain?
Following Moore’s law, How long before artificial neural networks can fully simulate a human brain?
When his back began hurting suddenly, Level Ex software engineer Tom Huffman assumed his bed needed upgrading and started looking at new mattresses.
Less than a month later, Tom collapsed at his home and was rushed to the emergency room. He messaged his supervisor, Whit Trebella, from the hospital to explain that tests were underway and later, to tell him about the tumor in his lung.
“It progressed very fast,” said Whit, Level Ex Core Team Lead Engineer. “He thought he’d be coming back to work soon and we talked about getting a beer, but then he was back in the hospital and intubated. It just kept getting worse.”
Doctors diagnosed Tom with a neuroendocrine tumor (NET), a cancerous tumor marked by its difficult detection and fast spread. Just weeks after the tumor was discovered, Tom died. He was 33.
After losing their friend and colleague, the Level Ex team was determined to honor Tom’s memory, while also raising awareness about neuroendocrine tumors (NETs) and taking action against the elusive disease. More than 90% of NET patients are incorrectly diagnosed initially, and patients visit an average of six health care professionals before the right diagnosis is made.
“Often, when someone passes from a terrible disease, people donate money to research. As a medical video game company, our team is in a unique position to contribute to this cause in a way that no one else can,” said Level Ex Founder and CEO Sam Glassenberg. “In our last company game jam, Tom Huffman and his team built what was almost a complete game about infectious disease. By setting up a game jam in honor of Tom, our team of the industry’s best video game developers, designers, and artists will contribute their skills to help doctors understand/diagnose/treat neuroendocrine tumors… so that perhaps we can help prevent the loss of incredible, talented people like Tom in the future.”
Tom Huffman, center, relaxes with Xinda Zeng, dog Chester, and Whit Trebella (left).
Starting on November 16, the team began hosting a company-wide Game Jam with neuroendocrine tumors as the target.
During Game Jams, a signature culture-builder at Level Ex, participants divide into teams across departments and over the course of three days, design video games from scratch. At the end, teams unveil their games for judging and a winner is chosen. In the past, teams have created a tower defense game focusing on the function of immune cells, a game where players fly through a bone implant and destroy bacteria, and a billiards game illustrating the spread of disease, among others.
For the upcoming jam, teams are focusing on ways to educate doctors on the complex symptoms and signs of NETs.
The NET Game Jam embodies the culture at Level Ex, said John Eberhardt, vice president of production at Level Ex.
“At the center of each of us, we want to make a difference and improve the world in which we live,” he said. “Games aren’t a vehicle to escape for us, they are another tool by which we can help save people. And when someone messes with our family, we don’t take it lightly – we look for something we can do about it.”
Colleagues remember Tom for his dry sense of humor, direct approach, and slight silly side. Before coming to Level Ex, he created his own games including, Dumpy: Going Elephants, a game where an escaped elephant smashes through objects with his trunk and Up Golf, where users play golf vertically and unlock goofy characters.
During his 4-year tenure at Level Ex, Tom was an integral part of countless projects, including building many of the features of Top Derm and implementing the registration flow still used in a number of our apps today.
If the disease had affected another of his colleagues, Tom would’ve jumped at the chance to participate in such a Game Jam, Whit said.
“I think he would’ve been all for it,” he said. “He would have dived right in.”
Tom during a recent camping trip with friends to Utah.
One of the highlights of a Game Jam is that it allows participants to take on roles they otherwise wouldn’t during traditional game development. Programmers can work on art. Designers can create sound. Tom was a game jammer that loved to amplify his contribution, working on programming, art, or whatever element was needed.
“Tom was a very humble person who did not enjoy being the center of attention, but he loved solving the problems we as developers, and our players as doctors, face,” John said.
With this shared passion, Level Ex hopes our efforts shine a spotlight on NETs and spur new ways of identifying and treating the disease.
“Unfortunately, this was something that was not caught in time. If it had been caught earlier, perhaps his chances of survival would have been higher,” Whit said. “We want to make sure this Game Jam helps get the word out about this disease and also promotes more ways of earlier detection. We owe it to Tom.”
We’ve all seen “that booth” before. The one at the conference buzzing with energy, with crowds swarming and attendees craning their necks to catch a glimpse of the mysterious magic inside.
And…we’ve all noticed that nearly-empty booth. The one that people walk swiftly past as the vendors pace and the candy bowl sits untouched.
What makes the difference between a lively healthcare conference booth and an unremarkable one? Does integrating games, VR, or AR do the trick? It’s not that simple. Take VR for example. A common misconception is that adding a VR experience to your booth will automatically draw the masses. In fact, some marketers have shelled out mega bucks to animation agencies that push VR only to learn from experience that this isn’t the case. The secret isn’t in the technology itself, but in how you use it.
Our team at Level Ex has built dozens of AR and VR experiences played by thousands of medical professionals across all specialties, including our latest spine surgery simulation that will debut at the 2022 North American Spine Show (NASS) in Chicago. We are one of a handful of health tech companies in an early access program for a key AR platform.
In this mixed reality experience capturing spine surgery, the spine stands solo on the table and actually changes color in response to the player’s decisions to elicit an intuitive understanding of the impact of each step. Sign up now to play our new Spine XR Experience at NASS.
Straight from our own playbook, here are 5 Do’s and Don’ts when creating a VR version of a medical procedure, technology, or software:
(Note these questions apply to any AR and mixed reality experiences but we’re using VR here for simplicity).
1. Do Create a Spectacle
Trying to attract a larger audience? Keep them in the booth longer? VR could be your ace in the hole, if you use it wisely.
Showcase what the user is doing. Make sure the crowd can see what the user can see, by broadcasting it on a big screen in front of them… and make sure that whatever they see is breathtaking—with high-quality graphics.
Get the player moving around. Take advantage of room-scale VR to get the player moving around a physical space. If you use a controller, make sure the player is encouraged to move it in interesting ways (grabbing, hammering, etc.). Yes—this makes a more visceral experience for the player, but more importantly—it also makes it more intriguing for audience members to watch. No two gameplays should be the same. Again, make sure the crowds can really see what’s happening. Make it intriguing so audience members can’t help but stop by.
In 2016, our team created some of the first headset-based VR experiences for physicians – even before the first Oculus officially launched. Our aim was to rally the crowd, and it worked. The devices drew the largest crowd of any booth at an anesthesia conference, despite a suboptimal booth location.
Since then, we’ve continually built conference booth headset experiences for ourselves and for clients using Oculus, Magic Leap, and others. On more than one occasion, we’ve had a client with the same booth location year-over-year at the same conference. This yielded a unique opportunity for a controlled study. We measured that the experience TRIPLED booth traffic, and measurably increased other key metrics like opt-in rate and time-in-booth.
Companies invest heavily in conference booths. When used correctly, VR can measurably increase ROI on that conference investment. Remember: be deliberate, make it worthwhile, and use its attributes to your advantage.
2. Don’t Just Replicate, Teach
The standard goal of most VR built for medicine is to teach – a skill, a technology, a treatment, how to care for a patient. If you’re just replicating in virtual format the same linear steps surgeons are already performing in their O.R., is that teaching anything? Most likely not, but that’s what a large majority of such experiences do: Pick up the scalpel. Find the location on the spine. Click to start. It’s a nice review and interesting, to see it in virtual form, but it’s not actually teaching anything new or anything very effectively.
How do you avoid this?
Consider what we did in our recent VR experience built for spine surgeons: take the spine out of the patient and toss it on the table to play with.
In all seriousness, it’s a neuroscience-backed approach honed from years in the video game industry. Here, we need the players (in this case, spine surgeons) to understand that even during high-precision workflows, the use of certain instruments can cause physical displacement of adjacent bones from where the navigation software has registered them to be. This can result in misaligned screw placement, but that is difficult to see in a minimally invasive procedure. So we strip the experience to the essentials—removing all the tissue, muscle, and skin that obscures the motion of the vertebrae—allowing players to focus on these critical details. We invite them to explore and experience it—the spine actually lights up in response to their decisions and interactions. We enable abstraction and creative thinking so they can intuitively grasp the challenge and develop a lasting mental model for the decision-making steps and device.
Another example is our Gastro VR experience where players can experience the visceral thrill of being the colonoscope. The captivating experience includes action–based objectives that help boost players’ skills and increase competency.
In this Gastro VR experience, players can scope, biopsy, snare, and APC in thrilling gastroenterology cases.
3. Do Extend Your Experience Beyond the Headset
VR is not the only entry point to immersive experiences. It’s not the pinnacle of medical simulations. True, VR headsets are especially great for conferences—they encourage traffic and conversation in your booth (that’s why we often have one in our own booths!) And they offer stereoscopic 3-D, their most valuable benefit. But anyone who wants to create a meaningful and memorable experience needs to ask: what happens when the surgeon walks away from the headset? From the booth?
At Level Ex, one of our guiding principles is that everything we build should be multi-channel—available across any device, anywhere, anytime. As a result, today surgeons across the world are collaboratively practicing complex cases remotely, on common platforms like Microsoft Teams or Zoom. Medical device companies are creating virtual versions of their technology and replicating a hospital site visit—instead of traveling from hospital to hospital (challenging even before the pandemic) or trying to explain multimillion-dollar equipment using a slide deck or videos.
Level Ex games have been played by over 800,000 medical professionals on their mobile devices. Over 80,000 have played our mobile AR content. Compare that to the 8,000 who’ve played our games on headsets—still a huge number—but it illustrates the two orders of magnitude you give up when limiting your experience to VR-only.
Do consider the limitations of headsets and recognize the other engagement possibilities beyond your booth.
4. Don’t Sacrifice Function for Flashiness
Certain scenarios and circumstances work better for VR than others. Video games are the poster-child for 3-D, but we don’t use the format all the time. We don’t have players navigate their avatars to a table at a 3-D casino and manipulate a bunch of 3-D cards to play Solitaire. The card game is better played in 2-D for convenience and a faster tempo.
Yes, VR headsets are especially great for conferences—they encourage traffic and conversation in your booth. Beyond this, it’s important to consider whether it helps teach the specific medical scenario or challenge we’re applying it to.
We have found that VR is especially effective for teaching procedures and skills that require spatial awareness. For example, room-scale VR can be effective when training healthcare professionals on techniques that require them to figure out the best way to position themselves relative to the patient or device, such as intubation or ultrasound-guided interventions. Sometimes however, VR is simply another layer to learn on top of an already complex procedure, unnecessarily increasing the cognitive load and detracting from the very learning objectives that are core to the experience.
5. Don’t Fall into These Common VR Traps
One of the worst offenses in VR is not taking advantage of the virtual space. I once sat in a VR experience where someone was reading off slides the entire time. I wondered why it wasn’t just a video. I wasn’t being asked to move about the space or look around the room—just to sit and watch a presentation.
An even worse offense is an experience that triggers dizziness or nausea. The last thing you want are audience members leaving your booth in worse shape than when they arrived. Our team of biomedical solution specialists and game designers understand the physiology of motion sickness and peripheral vision and how to design games that complement the interaction between our visual and vestibular systems instead of interrupt.
Another frequent mistake? Sitting a player down in an isolated egg chair, stuck in a corner away from the crowd. Avoid ‘lonely’ VR setups that are only experienced by the player with the headset on. The game alone isn’t the sole driver of traffic at a conference. When the audience sees a player actively interacting with and enjoying an “invisible” world, they want to experience it for themselves.
Be mindful not to slip into these VR sinkholes. Instead, ensure the experience is set up to really rally the audience. Make the experience high-energy and make it spectacular. Be “that booth” that everyone can’t stop talking about.
Schedule time with us at NASS 2022, your next conference, or anytime to play our mixed reality experiences or see how we can work together.
Over the past few years, thoracic oncology has made incredible gains on the treatment front. We can reap even greater benefits from these advancements by expanding screening efforts.
As Director of Bronchoscopy and Co-Director of the Lung Cancer Screening Program at University of Chicago Medicine, my mission is to advance cancer diagnostics and treatment. The work I do everyday is in service of this mission. Early stage lung cancer rarely has any symptoms, so it isn’t uncommon that by the time a patient presents with something that would lead to imaging, the cancer is usually advanced. Just recently, I screened a patient who presented with stage 2 lung cancer. They will need to undergo systemic treatment, so it’s imperative that I biopsy enough tissue in order to test for oncogenes and identify the appropriate therapies that the patient will need to achieve the best possible outcome.
Facts sourced from clinical trials in the US and Europe as well as CDC reports.
Because many tumors can now be treated with target drugs based on their genetic characteristics, Level Ex developed a game for the Pulm Ex app to simulate the experience of biomarker testing and raise awareness around the importance of identifying driver mutations at diagnosis to inform treatment options. Healthcare professionals to navigate a bronchoscope through the airways of a lung to remove biopsy tissue at the location of a suspected cancer mass. They can then experiment with different testing methods while reviewing the current biomarker testing recommendations and uncovering facts about one of the most common oncogenic drivers in non small cell lung cancer (NSCLC), KRAS G12C.
The KRAS G12C unit in Pulm Ex provides a closer look at the underlying mutations at the root of non-small cell lung cancer which are critical to developing an effective treatment course.
While it is clear that advancements such as targeted therapies and combination therapies have improved outcomes for advanced lung cancer, the fact remains that CT scanning can reduce cancer deaths by catching more cases early. Greater improvements are possible with continued research investment and increased use of screening advances. Here are my recommendations for expanding lung cancer screening in the US.
Improved Awareness and Education
In my role, I’ve experienced first hand the power of screening. Unfortunately, there is little awareness amongst patients—and doctors, to a lesser extent. Every year, there are widespread campaigns for breast cancer screening that convey the importance of early detection and demystify the process. These efforts have been successful in making breast cancer screening a more standard preventative healthcare measure. While it is common for a woman to have a conversation about breast cancer screening with her doctor, the same cannot be said for lung cancer screening. In fact, only 4.3% of all adults report having a discussion about lung cancer screening with their physician. We need to equip and empower both patients and physicians alike with essential information if we want to improve these numbers.
Quality Training and Enterprise Building at Hospitals
Screening begins with a low-dose CT (LDCT) scan of the patient’s chest to obtain a detailed image and analyze it for any abnormalities. For some, this quick, painless, non-invasive diagnostic test will be the first and last step. However, if further investigation is warranted, we can perform more in-depth bronchoscopy if needed to sample the lesion. Using advanced medical technology, we can explore deep in the periphery of the lung and get radiographic 3D views of the lung in real time to guide the instruments into the nodule or sample the lymph nodes inside the chest from inside the windpipe utilizing endobronchial ultrasound (EBUS).
Advancements such as robotic bronchoscopy, EBUS, and external imaging have made lung cancer screening a minimally invasive procedure if a biopsy is needed—much like a mammogram. It has also made screening more accurate and thorough. My clinic was an early adopter of this technology. Traditionally, adoption of new technologies into the medical field is a slow transition. There are fears, doubts, and of course, a learning curve. New tech requires change and a willingness to learn and adapt both for physicians and hospitals. This is one of my motivations for joining Level Ex as a physician advisor. I believe we can use virtual and game-based training to accelerate this adoption curve and shorten the learning curve. More practice in a high-fidelity training model helps make a physician more prepared for the real world. By providing quality, high impact training for medical professionals, we can ensure that more hospitals are providing this service and have the ability to help patients bronchoscopically that need samples taken from their lungs accurately and safely. This in turn benefits oncologists who will need that information to determine the best course of treatment.
The Sanguine Scourge game, in Pulm Ex, lets players practice removing squamous cell carcinoma with limited visibility. This is an opportunity to practice challenging procedures in a risk-free environment.
Reducing Barriers to Access
Awareness, education, and training efforts can help ease fear of the unknown, but there are other barriers—both mental and physical—that must be addressed. First, stigma. Lung cancer is viewed as a smoker’s only disease which can lead to feelings of shame or guilt which can delay or even prevent people from seeking treatment. There’s this stigma of “well of course you got lung cancer!” This attitude needs to be destroyed. Smoking is an addictive habit, with the biology of addiction similar to heroin and cocaine and it’s been well demonstrated how the tobacco industry markets to teens and children to get people hooked on cigarettes at an early age. While it is true that smoking can increase the risk of lung cancer, it is not the only cause and the number of non-smokers with lung cancer is growing. Regardless of a person’s history, everyone deserves quality care and compassion from a well-trained, competent, and empathetic physician.
Additionally, there are various logistical issues that deter patients from participating in screenings. For example, qualification criteria are difficult to understand and navigate. There must be clear and established guidelines for all. This recommendation summary from the US Preventitive Services Task Force is a helpful resource for patients and medical professionals alike.Once past that hurdle, it can be a challenge to find a facility. To address this issue, The American College of Radiology provides a lung cancer screening locator tool.
With continued efforts to improve education, training, and access for lung cancer screening, we can diagnose sooner and connect more patients to the life saving treatments they need to achieve the best possible outcome.
D. Kyle Hogarth, MD, is the Director of Bronchoscopy and Co-Director of the Lung Cancer Screening Program at University of Chicago. In addition to being an expert in pulmonary disease, he is involved with the minimally invasive diagnosis, management, staging and treatment of lung cancer through bronchoscopy. He was the first physician in the region to utilize the Auris Monarch platform, a robotic bronchoscope that allows deeper access to the lung without surgery as well as the LungVision system for 3D images of the lung during biopsies. He uses endobronchial ultrasound to biopsy lymph nodes, debulks central tumors, places stents in cancerous airways, and performs all other minimally invasive techniques to help patients with lung cancer. He is involved in several clinical trials that are investigating therapies for lung cancer that can be administered via the bronchoscope.
At Level Ex, Dr. Hogarth has advised on the development of Pulm Ex. His vision for the future of bronchoscopy includes integrating external radiology into scopes, advancing ablation/curative technology, and further development of virtual, game-based, and live model training for new technologies.
Think about the last time you had to learn something—really truly master a concept. Was it fun?
Maybe you had to study for a board exam. Maybe you had to understand market research for work. Maybe you had to understand basic geometry to help your kid with her homework.
Did you relish the experience? Did you lose yourself in it?
Chances are you did not. Chances are it wasn’t your definition of fun.
Now imagine a world in which learning of all kinds, across all ages, is actually delightful. You look up at the clock and realize you’ve lost track of time because you enjoyed what you were doing so much—and you learned.
Why isn’t this the norm yet?
Sure, there’s lots of talk about how to make education more engaging and enjoyable, and teachers think about this all the time when planning their curriculum. But as many of our own personal experiences will tell us, these are isolated incidents.
Which brings us to the answer to this question and the core of the problem— a fundamental flaw in how we think about learning and fun.
Educational value and fun have for too long been seen as two mutually exclusive ends of a spectrum, an either-or-dichotomy within individual learning opportunities: textbooks are for learning while video games are for off time. In recent years, there have been attempts to bring these types of activities together, for example adding quizzes to textbooks or “gamifying” teaching lessons by inserting mechanics like trivia or timed races. But this is just slicing the cake up differently— sprinkling a little “fun” there, breaking from learning for a little gaming here, and sometimes subordinating quality of content to fun or the other way around.
Instead, we should be duplicating the cake (yes, learning is so fun we can have our cake and eat it too). When we do this, 100% of the learning piece is fun and simultaneously 100% quality and education.
We need to turn our learning into games.
Across hundreds of studies, researchers have found significantly higher cognitive gains for training groups taught with interactive simulations and serious games6,9.
Games are truly effective – if not the most effective approach – for learning.
It’s especially noteworthy that gameplay is proven effective for improving adults’ work competencies, with studies demonstrating a 20% increase in self-efficacy, 14% and 11% better outcomes in terms of procedural and declarative knowledge, respectively, and nine percent higher knowledge retention rates7.
But why is that the case? There are three key psychological and neurological theories and evidence to explain this effect. Understanding them may be the key to instilling the confidence and insight we need to more fully adopt games as a learning method.
Accidentally Learning
I pledge allegiance to the flag of the United States of America,
and to the republic for which it stands, one nation …
Did your mind just automatically complete the pledge of allegiance said in classrooms across America since an early age?
Many of us have memorized these lines and we can easily reproduce this knowledge—without having studied it intentionally. We did not write it down, it wasn’t tested in an exam and we did not receive a grade, yet somehow we learned it anyway and it’s stuck in our minds for decades.
Why?
Learning is not limited to school. We learn every day of our lives—new exercise routines, the lyrics to our favorite songs, the name of our kids’ friends at school, or how to use a new coffee machine. Incidental learning, as in these examples, is just as efficient as intentional learning11.
This ability of the brain to learn something on the fly, accidentally, is part of what Level Ex taps into when it creates and releases video games for doctors. Rather than sitting down to consume incredibly important and dense material in the form of lectures, slide presentations, videos, and textbooks as has been the case for many years, medical professionals can pull out their phones to play a game. Instead of intentionally thinking “I am going to learn now”, they think “I’m going to have fun now”. But as they are playing, their minds absorb the information and build models for the skills they are practicing—just like yours does with the lyrics to your favorite song.
Flow into a Zone of Proximal Development
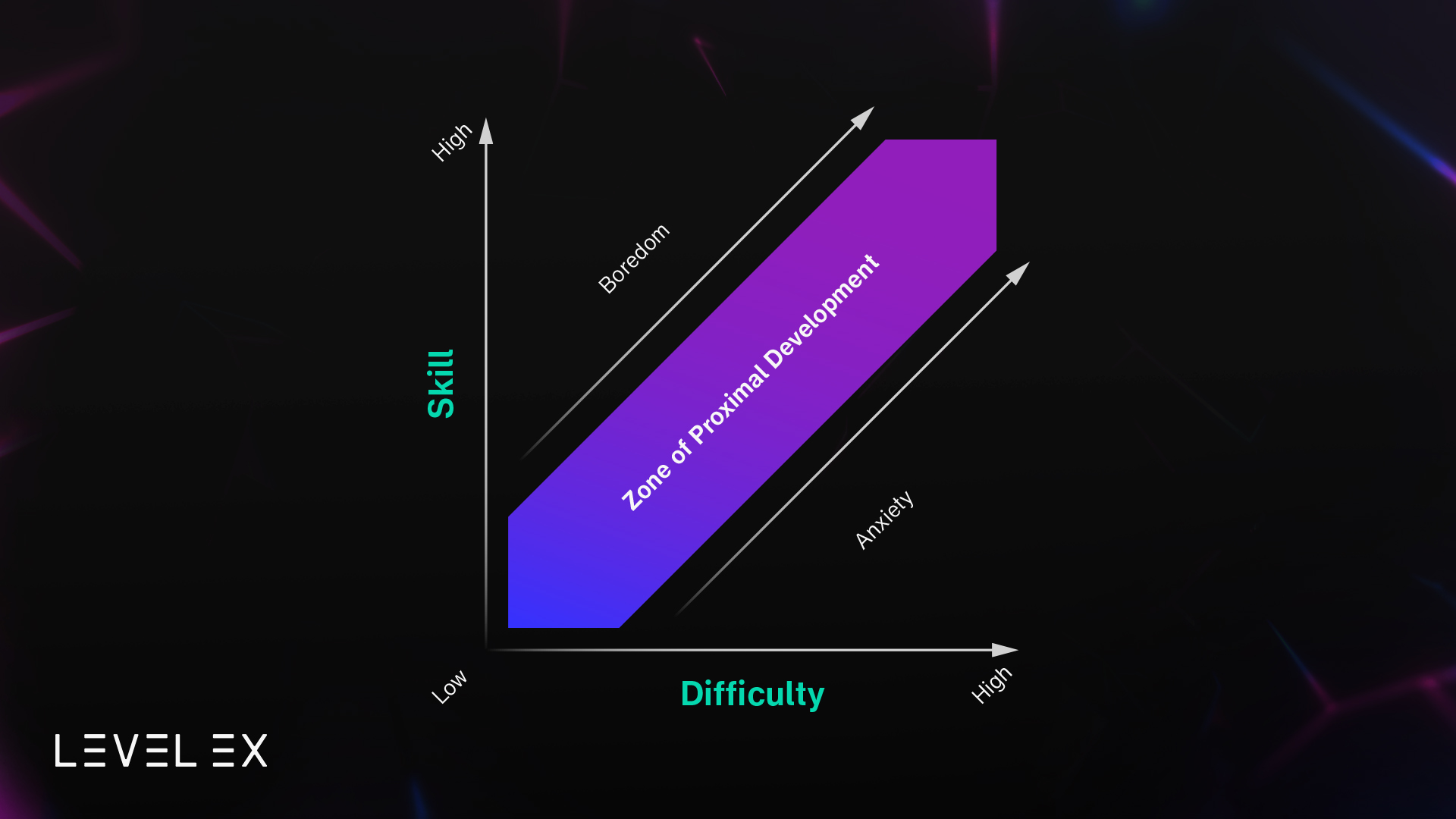
Somewhere between what a student already knows and what a student isn’t ready to learn, lies a “magic middle” that educational theorists refer to as the Zone of Proximal Development (ZPD)10. In short, the most effective and efficient learning happens when students are kept at the edge of their abilities. The tricky part is that this sweet spot differs greatly between learners. In other words, what’s just the right amount of challenge for one student might be absolutely overwhelming for another.
Effective teaching needs to aim for each learner’s individual Zone of Proximal Development, to adapt to different learning paces and preconditions. Doing this through conventional teaching methods? Practically unachievable. Doing this through video games? A piece of cake.
The concept of ZPD is in large part the secret sauce that game developers have perfected from years of creating games that have reached billions of people—billions of learners—all over the world. To teach players how to find the hidden gems in a cave, defeat zombies, or stent a beating heart before the clock runs out, games don’t alternate between ‘gaming’ and ‘learning’ or add on “fun” widgets. They do so by integrating it all into one experience that keeps players in the perfect balance of challenge and skill.
Did you ever sit down to do something you enjoy before bed and then suddenly notice the dawn breaking outside your window? What felt like a half an hour to you was, in reality, a day’s work. You didn’t get abducted by aliens or slip through a crack in the fabric of spacetime—you were simply in a heightened state of engagement.
This is the essence of Cognitive Flow3, a state of deep concentration and task absorption that makes a person feel at one with the activity. Since it provides the most beneficial environment for knowledge acquisition, any type of learning activity should aim to enable learners to enter this state of cognitive flow5.
Searching for Reward: The Neuroscience Behind Games
We’ve looked at the theories and features of games themselves that make them effective for learning. Now let’s go deeper inside the human brain.
The reward systems of the brain are a group of structures that activate whenever we experience something rewarding, such as eating a nice tasting food, sex, or drinking coffee. When exposed to such a stimulus, the brain responds by releasing an increased amount of dopamine. This neurotransmitter for reward and pleasure is then transported from the midbrain to the frontal lobes, the region responsible for high cognitive functions like thinking or planning1,2,8.
These dopaminergic pathways can be activated through what we refer to as interrogative goals, or a search for reward4. Driven by dopamine, this type of motivation aids in encoding, consolidation, and recall of relational representations of multiple aspects of the environment–that is, it creates long-lasting, embedded memories.
How are these neuroscientific concepts connected to games and learning? Games create interrogative goals that in turn activate reward pathways and thereby create relational long-term memories—which equals effective learning! Indeed, research has shown that “gamification encourages inquiry, collaboration, and the exchange of ideas while avoiding unwanted stress that affects students’ abilities, unlike other teaching tools”4.
In contrast, most people don’t exactly get a dopamine rush from a textbook.
So how can we get to a place where games are freely integrated into education as a modality for learning?
We need more interdisciplinary research to differentiate exactly what aspects make games effective for learning. We also need to start having more open conversations about the important role games play in learning and understand how and why they are so effective for learning.
Only then will we be able to overcome the mutual exclusivity of “learning” and “fun” and get to a place where learning is fun—a place where games have been accepted as an effective modality in education for all.
References
Arias-Carrión, O., Stamelou, M., Murillo-Rodríguez, E., Menéndez-González, M., & Pöppel, E. (2010). Dopaminergic reward system: A short integrative review. International Archives of Medicine, 3, 24.https://doi.org/10.1186/1755-7682-3-24
Csikszentmihalyi, M. (1991). Flow. Harper Collins.
Luria, E., Shalom, M., & Levy, D. A. (2021). Cognitive Neuroscience Perspectives on Motivation and Learning: Revisiting Self-Determination Theory. Mind, Brain, and Education, 15(1), 5–17.https://doi.org/10.1111/mbe.12275
Moneta, G. B. (2018). Cognitive Flow. In J. Vonk & T. Shackelford (Eds.), Encyclopedia of Animal Cognition and Behavior (pp. 1–5). Springer International Publishing. https://doi.org/10.1007/978-3-319-47829-6_1587-1
Riopel, M., Nenciovici, L., Potvin, P., Chastenay, P., Charland, P., Blanchette Sarrasin, J., & Masson, S. (2019). Impact of serious games on science learning achievement compared with more conventional instruction: An overview and a meta-analysis. Studies in Science Education, 55, 169–214.https://doi.org/10.1080/03057267.2019.1722420
Sitzmann, T. (2011). A Meta-Analytic Examination of the Instructional Effectiveness of Computer-Based Simulation Games. Personnel Psychology, 64(2), 489–528.https://doi.org/10.1111/j.1744-6570.2011.01190.x
Tritsch, N. X., & Sabatini, B. L. (2012). Dopaminergic Modulation of Synaptic Transmission in Cortex and Striatum. Neuron, 76(1), 33–50.https://doi.org/10.1016/j.neuron.2012.09.023
Vogel, J. J., Vogel, D. S., Cannon-Bowers, J., Bowers, C. A., Muse, K., & Wright, M. (2006). Computer Gaming and Interactive Simulations for Learning: A Meta-Analysis. Journal of Educational Computing Research, 34(3), 229–243.https://doi.org/10.2190/FLHV-K4WA-WPVQ-H0YM
Vygotsky, L. S. (1978). Mind in society: The development of higher psychological processes. Harvard University Press.
Hundreds of doctors and healthcare experts across specialties work with the Level Ex team, developing games that advance knowledge and skills in medicine. Like Level Ex, a group of these highly active advisors are on a mission to help ‘play’ take its rightful place among other modalities of learning – such as lectures, conferences, videos, journals and textbooks – a mission to make training and education better for healthcare professionals (HCPs) and industry.
At the first Level Ex Medical Advisor Meeting of 2022, these forward thinkers and leaders in their field came together to discuss this mission. What new and yet-to-be-released technology will have the most impact and where is the greatest need? Which specialities are especially in need of game technology? Here’s an inside look at the top five ways our advisors say games will shape the future of ongoing medical education.
1. Accelerating the adoption curve of new skills in medicine
Right now, most HCPs rely on existing modalities of education — live videos, animations, and lectures —to better understand novel concepts, from using the latest ablation system or understanding the mechanism of action of a new drug class. These methods are important, but studies consistently show play is highly effective at helping people develop mental models to understand complex concepts.
“By 2027 we envision a world where play is broadly accepted as a fundamental force accelerating the adoption of new skills in medicine. We want it to be the universally accepted best practice,” says Sam Glassenberg, Founder and CEO, Level Ex. Within the next five years, video games will be the go-to medium for scenarios where a physician needs to deeply understand a complex system.
2. Engaging healthcare professionals across the industry
Much of the latest and exciting tech in healthcare is geared toward doctors, from robotic surgery to VR. However, non-physician healthcare professionals also need more engaging and effective methods of medical training.
“I think that the targeting of physicians is great and it’s important, but we should not miss everyone else in healthcare — nurses, paramedics, technicians,” says Dr. Rafael Grossmann, MD, FACS, Healthcare Futurist, Technology Innovator, Surgeon & Educator.
Pediatric Cardiologist Dr. Shawn Sen, MD, Assistant Professor of Pediatrics (Neonatology) and Pediatrics (Cardiology) at Northwestern University Feinberg School of Medicine says he was brought up to value all the different roles in healthcare — from nursing to social work – and believes game technology can unite experts across the care team. “There’s such a push for interprofessional team atmosphere and healthcare cooperation,” he says.
3. Creating a consistent and strong foundation with residency and fellowship programs
While HCPs successfully use games to advance their skills and master complex and rare cases throughout their careers, games are an especially effective modality for teaching foundational medical concepts. From the Krebs cycle to common disease interactions, this makes games a good fit for training programs like fellowships and residencies, in addition to the critical role they play in Continuing Medical Education (CME) and Continuing Professional Development (CPD).
“Games can be very useful in tackling complex concepts that are useful to health care —things like genetics and informed consent,” says Dr. Komal Bajaj, MD, MS-HPEd, Chief Quality Officer at NYC Health + Hospitals/Jacobi.
Dr. Sen agrees. “I can’t tell you how painful it is to run a simulation code with dummy models meant to represent real humans,” he says. “I have trainees who can’t take it seriously because it just doesn’t seem real. To be able to really show what it’s like to experience this at the bedside, to practice making your own medical decisions – that would be so incredibly helpful.”
Incorporating game technology into medical education at this level also builds a consistent and effective foundation for trainees and improves access to high quality education. Trainees develop lifetime strategies, habits, and approaches at this stage, but not all have the same access or opportunities. Creating that foundational conceptual understanding and exposure to new techniques and devices broadens trainees’ skill set beyond their home institution.
4. Breaking down generational barriers
Nearly all of the advisors had faced the misperception that video games in medicine were for younger generations. But the value of applying game technology to medical education is not only effective and enjoyable for all learners, but is actually already used by healthcare professionals of all generations. It’s important, the advisors say, not to reinforce such thinking that can therefore discourage HCPs who might otherwise be interested in using play as a modality of learning.
“If we’re losing [the opportunity to train] our physicians in their 50s and 60s, we’re losing decades of expertise,” says Dr. Sen.
“Short but meaningful ‘micro-learning’ experiences have been found to be much more effective for all learners because they let you train at your own time and your own pace,” says Dr. Eric Gantwerker, MD, MMSc, Pediatric Otolaryngologist at Cohen Children’s Hospital at Northwell Health/Hofstra and VP, Medical Director at Level Ex. “It’s much better than being at a conference for five days or sitting through five hours of lectures, which is often what healthcare professionals at all phases of their careers need to do in our traditional system.”
5. Prioritizing patient safety
Given the ability to earn CME credit for Level Ex games, the steady increase in players, and ongoing efficacy studies that validate games as a modality for learning, the day is not far off when patients will see the value of medical professionals who have used games to learn as well.
“The idea of doing a real focused practice on things that are so low stakes but allow us to do things that we had otherwise needed patients to help us with before, is beyond invaluable,” says Dr. Anthony Klappa, MD, Cardiologist at Washington Regional Medical Center.
Both medical students and physicians with decades of practice need to refresh their skills every now and again, especially when it comes to rare and challenging cases that they may not see on a daily, or even yearly, basis. With medical training games, HCPs can fine-tune their skills before entering the OR.
“The idea of ‘don’t practice on me, practice on a game first’ is really, really powerful,” says Dr. Bajaj.
5G will revolutionize the mobile phone experience for consumers and healthcare professionals alike—here’s how to sort out the hype from reality in 2022.
Let’s start with consumers. You’ve been told 5G will be revolutionary, but something doesn’t sit right with you. It usually goes something like this:
“What’s the killer app?” you ask.
“You’ll be able to stream HD video to your phone!”
“Hold on. I can stream HD video to my phone on 4G.”
“Well, you’ll be able to … stream 8K video!”
“8K video on my five-inch phone? I’ll need to upgrade my eyeballs.”
The truth is that there is a resounding 5G breakthrough app for consumers: cloud gaming. With it, you can play high-end AAA games on your phone that would normally only play on a $3,000 gaming PC. You can feel the lightning speed at which the game’s action responds to your movements on the touchscreen. How? The game is not really running on your battery-powered phone.
Thanks to low-latency 5G (and the infrastructure investments from wireless providers to deploy it), the graphics and physics are computed on a high-end computer running hot in the cloud, but to you (and your friends playing remotely with you), the lag between phone and cloud is imperceptible.
As it turns out, 5G does have a killer app for healthcare in 2022 … and it looks a lot like the consumer killer app.
Healthcare professionals: You’ve been told 5G is about to revolutionize healthcare, but something about that doesn’t sit right. Your allergy to hype and buzzwords is flaring up.
“What’s the killer app?” you ask.
“It’s telehealth! And telerobotics! With low-latency 5G, a surgeon at Stanford will perform surgery on a patient in Georgia!”
I’ll tell you something that you may have suspected: 5G’s healthcare killer app in 2022 isn’t telehealth or telerobotics. Let’s break that down.
Telehealth
The truth is 5G doesn’t really address telehealth’s challenges because its limiting factor isn’t network bandwidth or latency.
The challenges lie elsewhere.
Most doctors have trained all of their careers to recognize and treat patients in vivo. Suddenly, they are expected to transfer their skills seamlessly to remote video? Imagine a dermatologist, for example, trained to diagnose a skin condition under ideal lighting conditions in the clinic. Now she struggles to do so from a selfie a patient sends from a smudged phone camera. This problem isn’t solved by network bandwidth—although it can be solved by deliberate training.
Telerobotics
Telerobotics over 5G is likely years away from any sort of regulatory approval. While remotely-operated robotic-assisted surgery (in which the surgeon is in the same room as the patient, but operating from a console a few feet away) is taking hold in certain specialties, we’re far from being able to do it reliably from any meaningful distance. In my own experience attending robotic cardiac procedures, I’ve twice witnessed the surgeon struggle and give up on the robot halfway through and open the patient’s chest the old-fashioned way.
This isn’t an option over 5G. Eventually, 5G robotic surgery will reach its potential, allowing doctors to perform surgery from miles (or oceans) away. But to make this happen successfully, we are going to need more training—remote operator training to manipulate the robot more effectively in a wider range of unforeseen scenarios and better training for on-site staff for when things don’t go as planned.
Good news: The 5G killer app for healthcare in the short term is training. Collaborative medical training—using cloud gaming technology. The same killer app for consumers is going to dramatically benefit doctors and patients.
Let’s step into an online multiplayer game like Fortnite. As a player, you are running around at around 20 miles per hour. At that speed, if you shoot a virtual paintball on-target with 100 milliseconds of latency on a 4G connection, you’ll be two meters off—a total miss. With 5G’s latency of less than 30 ms, you can actually play the game.
Now say the game in the cloud is a surgery simulation and the players are surgeons. In the OR, things (hopefully) aren’t moving at 20 mph, which is why cloud gaming tech can handle many medical scenarios over 4G connections today (e.g., simulating knee surgery). That being said, there are scenarios that simply can’t be simulated over 4G. With 5G latency of less than 30 ms and unlimited compute power from the edge or cloud, the complex fluid and tissue interactions in any surgery or procedure can be simulated. An interventional cardiologist can place a stent in a live, beating, human heart and the latency will be imperceptible. Multiple surgeons can collaboratively cut tissues or cauterize spraying bleeds on the same virtual patient in real time, from different locations, over Zoom or Webex.
The better news: We don’t need to wait for it. This technology is in use today. And in 2022, we predict surgeons in almost every specialty will start training on it.
Many top medical device companies have training modules live or in development that will allow surgeons to practice the optimal use of their devices across almost every major surgical and procedural specialty, including orthopedics, robotics, ophthalmology, cardiology, urology, neurosurgery, and radio-oncology.
In this 5G world, rather than building $50 million-plus simulation centers, hospitals and health systems can use this technology to create customized, flexible training available on their staff’s mobile devices or VR/AR headsets. 5G will deliver a handheld simulation center in their pockets with more compute power than all of the world’s physical medical training centers combined. In turn, doctors can train collaboratively, earning continuing education (CME) credit, while safely preparing for the most high-risk and difficult situations—situations they otherwise would only encounter on live patients.
We should all be excited about the future of telerobotic surgery and better telehealth. In the meantime, healthcare workers can pick up their phones and get ready to play. 5G’s medical training revolution is waiting for them.